Want to learn about an interesting variant of Wet Age-Related Macular Degeneration (AMD)? Let’s talk about retinal angiomatous proliferation (RAP). Unlike choroidal neovascularization (CNV), which starts in the choroid, RAP starts in the retina. The neovessels then proliferate toward the choroid, forming a subretinal lesion and eventually breaking through the retinal pigment epithelium and invading the choroid. Varying classification schemes have been proposed and RAP is popularly called type 3 neovascularization (we’ll cover types 1 and 2 another time).
In a recent publication by Ravera et al, the authors took a fresh look at some previously documented findings. They evaluated the multimodal features of this pathology with particular attention to OCT identification.
| RAP | Other CNVs (not RAP) | p-value | |
|---|---|---|---|
| Presence of intraretinal cystoid lesions | 100% | 14% | <0.01 |
As you can see from the table above, the authors detected intraretinal cystoid lesions (ICLs) in 100% of RAP cases. Compare this with non-RAP cases, where they only detected 14% ICLs. Yes, there are limitations to this study (small sample size, etc.), but the findings are consistent with other publications: you can expect more ICLs in RAP than other types of CNV.
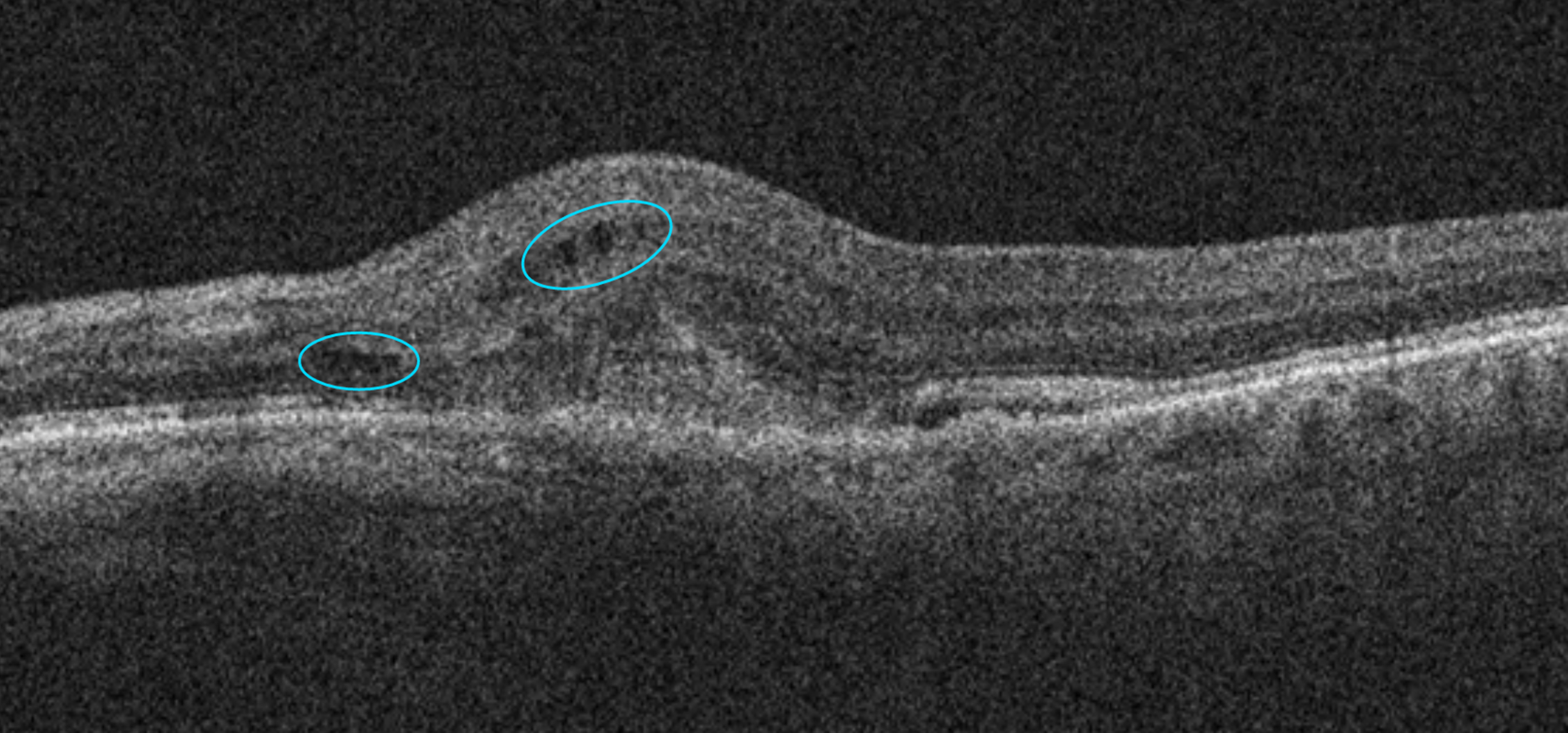
This image shows ICLs in a patient with AMD.
Early RAP lesions demonstrate an excellent response to intravitreal injections of anti-VEGF medications. But what’s even more significant is the fact that the vast majority of patients with RAP in one eye will develop RAP in the fellow eye within three years. So here’s what we recommend… increased surveillance, both at home and through in-office OCT testing.
Let’s wrap it up with a reminder that when evaluating the fellow eye, look for ICLs as an early marker of RAP—subretinal fluid, subretinal hyperreflective material and pigment epithelial detachments all indicate that you missed the early lesion.
Always learning,
The EyeCarePD Team